


Post-vaccine adverse events in Japan: evidence of racial differences?
A review of the literature

Although there’s no evidence that cultural factors reduced Japan’s Covid deaths, a new must-read paper on post-vaccination adverse events presents evidence that one of Japan’s cultural factors (nightly baths) increased its post-vaccination deaths!

The authors state that “The exact relationship between bathing and COVID-19 vaccination is unknown. However, there have been many sudden deaths while bathing after vaccination in Japan (50 cases; 29 females, 58% and 21 males, 42%; median age 80 (IQR 73–86) years).”
Of course, they conclude that to avoid dying, you should avoid baths in the days after your mRNA jab. I can think of something else you could avoid too.
So what does the rest of the scientific literature have to tell us about adverse events after mRNA vaccinations [1] in Japan compared with other places?
Reactogenicity
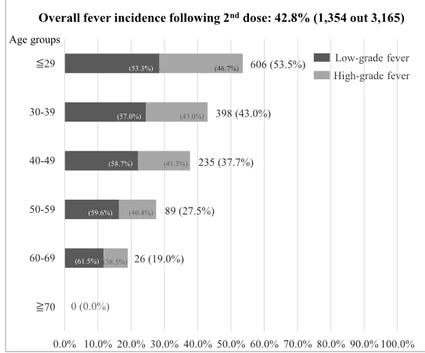
Saita et al. reported the results for reactogenicity among 3254 healthcare workers jabbed with Pfizer. Younger age groups reported adverse events at much higher rates.
Females also had significantly higher odds of suffering each side effect, specifically being about 2.5 times more likely to suffer headaches and 2 times more likely to suffer joint pain.

Comparing their results with those of an American study, they find reactions to be “much higher following the first dose (injection site reactions: 91.3% vs 65.4%; systemic reactions: 75.1% vs 48.0%) and second dose (injection site reactions: 92.1% vs 68.6%; systemic reactions: 86.8% vs 64.2%)” (emphasis mine). Er, aren’t those differences a bit concerning?
And it gets worse. Saita et al. also find “higher rates of these systemic reactions in our healthcare workers in Japan: fatigue (72.8% vs 47.8%), muscle ache (64.3% vs 36.8%), and fever (42.8% vs 21.5%).”
And before anyone says “Meh, that’s nothing”, we should probably see how debilitating these events were.
In total, 14 people (0.4%) were so ill they had to take more than a week off work. I’m pretty sure for young Japanese, Covid would probably be more pleasant.
One case of anaphylaxis was reported after each dose (both cases were females). These rates for the first and second doses (0.031%) were similar to those of another US study (0.027%). But when you consider it’s a two-dose series and the events were only among women, the anaphylaxis rate among females was 0.1% or about 1 in 1000 overall.
From all this, Saita et al. say that “severe cases were limited”, which is one way of putting it I suppose.
They conclude that “This study provides real-world evidence for the general population and organizations to prepare for BNT162b2 mRNA COVID-19 vaccination in Japan and other countries in the region.” They don’t clarify how the organisations should prepare, but presumably they shouldn’t jab the workforce when they need everyone to be at the office over the next week.
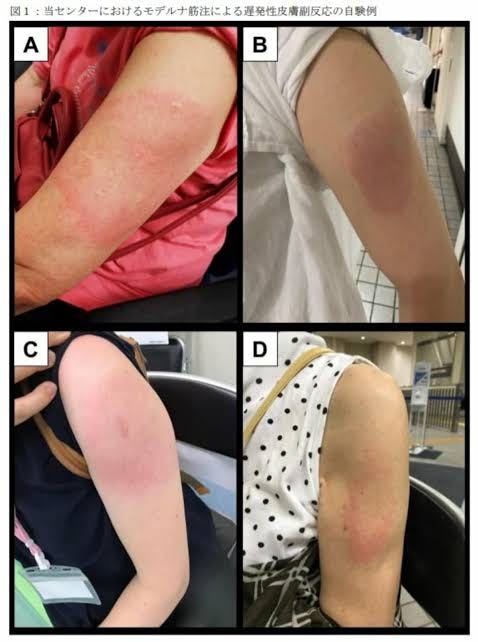
Moderna Arm
But there is one adverse reaction that is less prevalent in people under 30: Moderna arm, otherwise called a delayed large local reaction (DLLR) after the Moderna jab.
But unfortunately for Japanese ladies, they get it 5.3 times more than the gents: 22.4% vs 5.1%. And women of a certain age (40-49) get it the most.
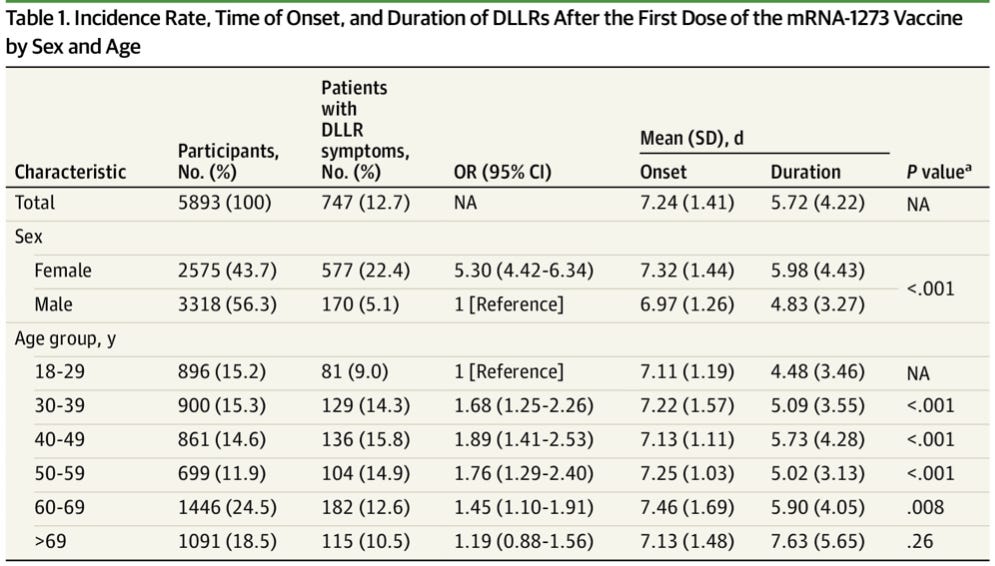
Why is it worse for females? The study authors, Higashino et al.. suppose that “Sex differences in body weight and immune responses associated with hormonal and environmental factors may partially explain the differences in susceptibility, time of onset, and duration of DLLR.”
And how do these results in Japan compare with those in the west? Higashino et al. cite studies that reported “cumulative incidence rates of 1.1% among female recipients in the US (no DLLR symptoms among 675 male recipients) and 0.16% in the general population in Germany.” A bit lower than 22.4% then. They offer the following as a possible explanation: “The difference in the incidence rate in our study compared with others is possibly attributable to Japanese recipients being more aware of skin symptoms after vaccination.” I’m as convinced as you are.
Deaths
But sex differences in adverse events aren’t limited to headaches and nasty rashes. Looking at reported post-vaccination deaths among people over 65 in Japan, the US, and Europe, Yamashita et al. found the ratio of female-to-male deaths followed a simple linear regression in Japan but not in the US or Europe. Put simply, more women than men were reported to have died in the first 10 days following the jabs in Japan, but the trend reversed after that.

So why were more women reported to have died soon after the shot? Yamashita et al. point out that adverse events may depend on the dose of the jab and the weight of the person being jabbed. This matters because the “body mass index in the Japanese female population is smaller than in the US and European countries.”
There probably isn’t a more logical explanation than that. The data suggest that Moderna’s jab has longer-lasting effectiveness and higher rates of adverse events than Pfizer’s due to higher dosage.
This dose/BMI relationship probably explains some if not most of the difference in reported reactogenicity between American and Japanese healthcare workers mentioned above.
When you think about it, this is quite ironic. The lower average BMI of the Japanese population is both one of the main reasons they suffer worse reactions to the mRNA jabs and one of the main reasons they never needed the jabs in the first place.

So is there anything in particular that Japanese women should worry about mortality-wise?
Thrombosis and intracranial hemorrhage
In May 2021, Shimazawa and Ikeda noted that of the first 10 reported post-vaccination deaths in Japan (5 males/5 females), four women died from intracranial hemorrhage (ICH, i.e., bleeding within the skull) but no men did. The women were aged 26, 61, 69, and 72 and died 3-9 days after the first dose. After clearing their throat with the standard “benefits outweigh the risk” line needed to get through peer-review, they conclude “we believe that a causal link with the vaccine is not proven but possible and warrants further analysis.”
Since the government ignored this flashing safety signal and proceeded with the mass-vaccination campaign, Okada et al. were able to conduct further analysis on 746 post-vaccination deaths reported to the Ministry of Health, Labour, and Welfare up to July 2021. They also found not only that “the proportion of deaths due to bleeding or intracranial hemorrhage was significantly higher in women, especially in those under 65 years of age” but also “death from cranial hemorrhage among young women was statistically higher than that among elderly women [frequency of death by cranial hemorrhage: 38.1 vs. 6.7%]” (emphasis mine).

So among women under 65, only 6.6% of all deaths in 2018 were from ICH but 38% of reported post-vaccination deaths were. This is a safety signal so bright even Stevie Wonder couldn’t miss it. But don’t worry, girls- it’s rare!
Japan even has a celebrity example: TV personality and doctor Ayako Nishikawa, who suffered an cerebral hemorrhage aged 50 in August 2021.
 - Yahoo!ニュース")
She survived but had to spend 4 months in hospital. In response to SNS comments that the jab was the cause, she responded on Instagram that “It’s known from many studies that the mRNA vaccines I took don’t increase the frequency of cerebral hemorrhages, so please don’t worry if you’ve been vaccinated. The main causes of cerebral hemorrhages are high blood pressure and changes in blood pressure.” Well, she is a doctor after all. But bear in mind she said this in October, shortly after Okada et al.’s paper had been published and five months after Shimazawa and Ikeda had pointed out the potential link.
Although they don’t try to explain the reason non-elderly women are more at risk, Okada et al. point out that “clinical data have demonstrated that bleeding is more prevalent in the East Asian population. It is therefore clear that the risk-benefit ratio of vaccines would differ from that in the Western population.” At this point, the risk-benefit ratio for the East Asian population is looking a bit lopsided.
All in all, the side effects of the government’s preferred pharmaceutical interventions against Covid have not been nice for the Japanese. And the side effects of the non-pharmaceutical interventions have been pretty rough too.
[1] Japan has used almost only mRNA vaccines, although it did administer 110,000 doses of AstraZeneca. I describe the Japan-AZ saga here.