


Why has Japan had so few Covid deaths (Part 4)? Was it immunological factors?
TL:DR Probably

So if mindo, mobility, and masks don’t explain Japan’s low Covid death count, then what does? To be honest, nobody knows for sure and there’s unlikely to be only one X Factor, but this post will look at six factors that evidence suggests have probably contributed.
Obesity is a well known risk factor for Covid. So it’s not surprising that, in an analysis of 168 countries, Foo et al. found that “For every 1% increase in obesity prevalence, the mortality rate was increased by 8.3%.” In 2016, Japan had an obesity rate of 4.4% compared with 37.3% in America (source)…

…which makes it strange that Japan originated a sport only for fat guys.

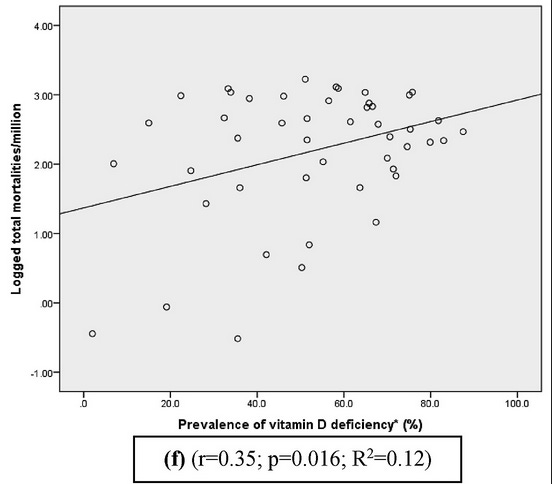
Another known risk factor is vitamin D deficiency. Sooriyaarachchi et al. found a significant association between vitamin D deficiency and Covid mortality in an analysis of 47 Asian and European countries. Japan was reported to has a lower than average vitamin D deficiency rate of 28.2%.
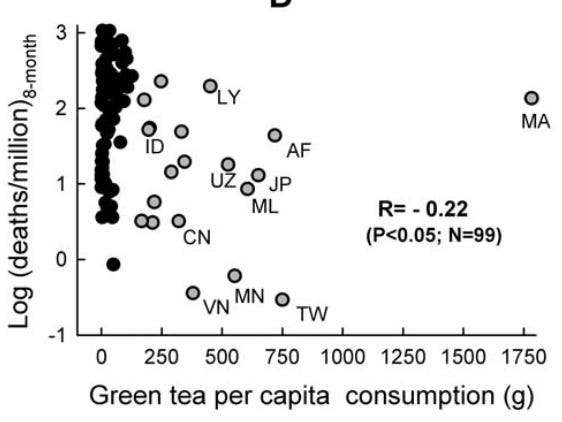
A lesser known factor appears to be green tea consumption. Storozhuk analyzed 134 countries and found “Striking differences in COVID-19 morbidity and mortality between groups of countries with ‘high’ and ‘low’ green tea consumption.” This may sound surprising, but these results were “in line with emerging evidence from other studies including pharmacological ones.” Needless to say, Japan (JP) was in the high consumption group.
Various researchers such as Klinger et al. have found an association between BCG vaccination coverage and Covid mortality. This has led researchers to suggest that BCG vaccines, which are primarily used to protect against tuberculosis (TB), help to train the immune system to respond to other viruses. [Update: There is now RCT evidence that the BGC Tokyo strain is protective against Covid. See my post here.]

But Inoue and Kashima suggested that this association is actually due to past rates of TB infections: countries with higher TB burdens had higher rates of BCG vaccination. Their reasoning is that “After latent infection, Mycobacterium survives in the human body and may continue to stimulate trained immunity”, which leads to countries with higher TB burdens in the past having lower Covid burdens now (like Japan).

Specifically for Japan, Shimizu et al. studied cross-reactive cellular immunity from past infections of seasonal coronaviruses. Because their study is highly technical, I’ll lazily quote from the popular press article about it.
The research team focused on immune type “A24,” which is present in 60% of the Japanese population, but only 10% to 20% of Western populations. The team analyzed the peptides that appear when individuals with immune type A24 are infected with COVID-19, and how killer T cells react.
As a result of this research, the team found that killer T cells react to COVID-19 infections highly efficiently due to a peptide called “QYI.” When cells of individuals with the A24 immune type, who had not been infected with COVID-19 virus, were collected and QYI was administered, killer T cells reacted and proliferated in 83.3% of them.

I think all these factors have protected Japan, although I’d say the last one may have contributed the most. But all this leads to another question: why has Japan had more Covid deaths in 2021 so far than in the whole of 2020? I guess that’s a riddle wrapped in an enigma.

Update 10 June
This series now has a fifth part.